

Abstract
Introduction:Patients undergoing cardiac surgery are among the most common recipients of allogenic red blood cell (RBC) transfusions. However, whether restrictive RBC transfusion strategies for cardiac surgery achieve a similar clinical outcome in comparison with liberal strategies remains unclear.
Methods:We searched PubMed, Embase, the Cochrane Collaboration Central Register of Controlled Trials, and conference proceedings from inception to December 2017 for all randomized trials (RCTs). The primary outcome was mortality. Secondary outcomes were stroke, respiratory morbidity, renal morbidity, infections, myocardial infarction (MI), cardiac arrhythmia, gut morbidity, reoperation, intensive care unit (ICU) length of stay (hours), and hospital length of stay (days). We calculated the risk ratios (RR) and weighted mean difference (MD) for the clinical outcomes using a random-effects model.
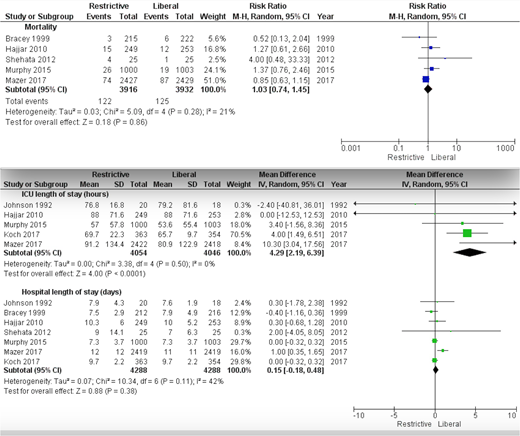
Results:We included 9 RCTs with a total of 9,005 patients. There was no significant difference in mortality between groups (RR 1.03; 95% CI 0.74-1.45; P=0.86). In addition, there were no significant differences between groups in the clinical outcomes of infections (RR 1.09; 95% CI 0.94-1.26; P=0.26), stroke (RR 0.98; 95% CI 0.72-1.35; P=0.91), respiratory morbidity (RR 1.05; 95% CI 0.89-1.24; P=0.58), renal morbidity (RR 1.02; 95% CI 0.94-1.09; P=0.68), myocardial infarction (RR 1.00; 95% CI 0.80-1.24; P=0.99), cardiac arrhythmia (RR 1.05; 95% CI 0.88-1.26; P=0.56), gastrointestinal morbidity (RR 1.93; 95% CI 0.81-4.63; P=0.14), or reoperation (RR 0.90; 95% CI 0.67-1.20; P=0.46). There was a significant difference in the intensive care unit length of stay (hours) (MD 4.29; 95% CI: 2.19-6.39, P<0.01) favoring the liberal group. However, there was no significant difference in the hospital length of stay (days) (MD 0.15; 95% CI -0.18-0.48; P=0.38).
Conclusion:This meta-analysis showed that restrictive strategies for RBC transfusion are as safe as liberal strategies in patients undergoing cardiac surgery.
Key points:
Restrictive strategies for red blood cell transfusion are as safe as liberal approaches in patients undergoing cardiac surgery.
Longer duration of stay in the intensive care unit is more common in patients managed with a restrictive transfusion approach. However, the overall hospital length of stay appeared to be similar between both groups.
Further studies are needed to ascertain threshold triggers for RBC transfusion.
Hassan:abott: Other: grant. Bhatt:American Heart Association Quality Oversight Committee: Other: chair; Boston VA Research Institute, Society of Cardiovascular Patient Care, TobeSof: Membership on an entity's Board of Directors or advisory committees; Medscape Cardiology: Consultancy; Regado Biosciences: Consultancy; Elsevier Practice Update Cardiology: Consultancy, trustee; cardax: Consultancy; Abbott, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, Eisai, Ethicon, Forest Laboratories, Idorsia, Ironwood, Ischemix, Lilly, Medtronic, PhaseBio, Pfizer, Regeneron, Roche, Sanofi Aventis, Synaptic, The Medicines: Research Funding; Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic, Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine, Population: Other: Data monitoring committee; American College of Cardiology; Unfunded Research: FlowCo, Merck, PLx Pharma, Takeda.: Other: trustee; ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim), Belvoir Publications (Editor in Chief, Harvard Heart Letter),: Other: board member; American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal